



The stakes, in one paragraph
Healthcare software development in 2026 is a compliance problem before it is a coding problem. The Change Healthcare ransomware attack of February 2024 hit 192.7 million people — the largest health-data breach on record — and cost UnitedHealth about $3.09 billion for 2024. The entry point was a remote-access portal with no multi-factor authentication. That single missing control is why regulators, buyers, and hospital security teams now treat compliance as the first design constraint, not the last. This is the map we hand every engineer who joins a healthcare build at Fora Soft: what applies, what it costs, and where teams get burned.
Key takeaways
- Design for the strictest regime in your footprint. HIPAA plus GDPR plus SOC 2 Type II covers most builds; FDA SaMD stacks on when the software makes clinical decisions.
- The 2024 HIPAA Security Rule changes are proposed, not final — but MFA and encryption everywhere are already table stakes. Build as if they are law.
- AES-256 at rest, TLS 1.3 in transit, keys in a dedicated KMS with rotation and access logging.
- Audit logs across app, OS, database, and network, retained six years. HITRUST is the strongest signal to hospital buyers; SOC 2 Type II is the floor.
The 2026 regulatory map for healthcare software
Most healthcare products get hit by four regimes at once. HIPAA applies the moment you touch US patient data. GDPR applies if any EU resident is in the system. FDA rules and 21 CFR Part 11 apply when the software diagnoses, treats, or drives a clinical decision. EU MDR with EUDAMED registration applies if you sell a device in Europe. State rules stack on top: California CMIA, New York SHIELD, Texas HB 300, plus every state’s medical-licensing regime for telemedicine.
The move that saves months is picking the strictest regime in your footprint and letting the others fall out for free. For most of our clients that means HIPAA plus GDPR plus SOC 2 Type II as the baseline, with FDA validation layered on only when the product is a clinical tool. Figure 1 shows which regime each trigger pulls in, and what each one demands in 2026.
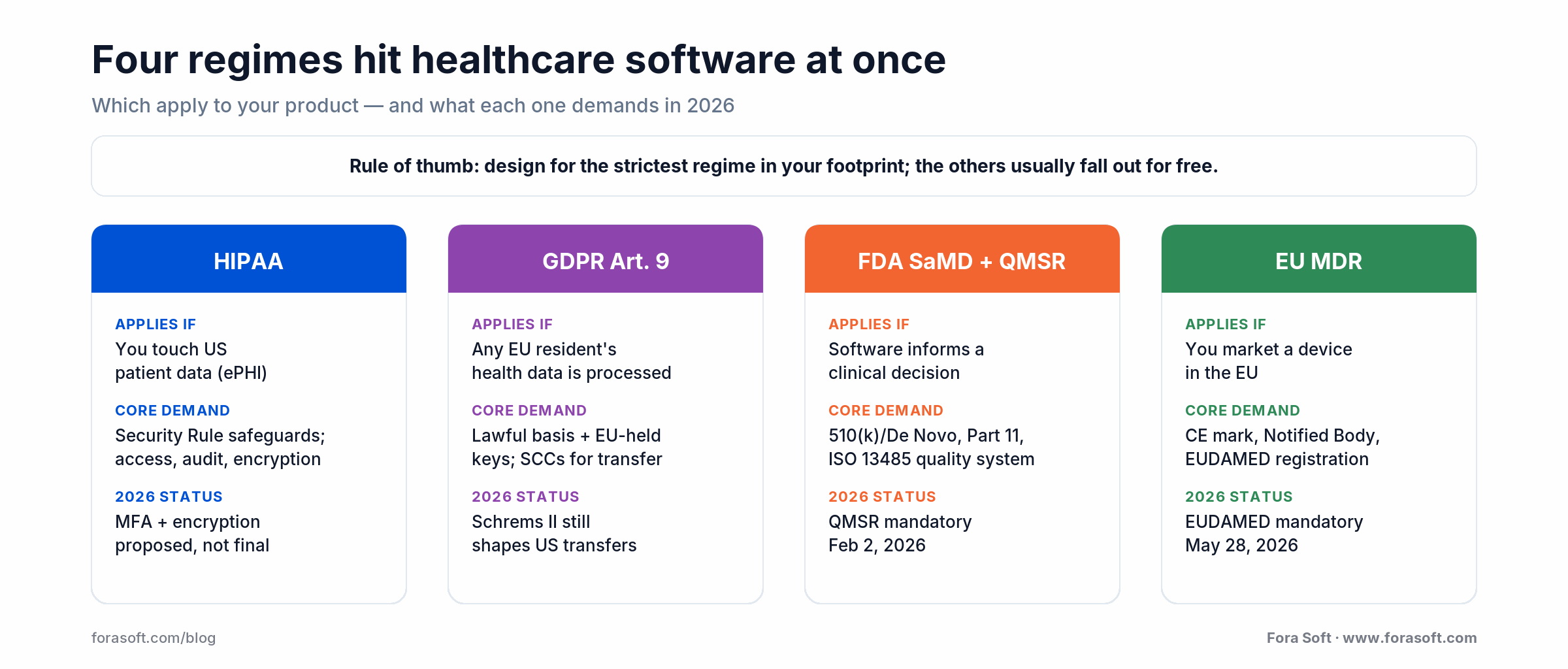
Figure 1. The four regulatory regimes that apply to healthcare software, and what each demands in 2026.
The proposed HIPAA Security Rule you should plan for
Is the big HIPAA Security Rule rewrite in effect yet? No. HHS published the Notice of Proposed Rulemaking on December 27, 2024 (Federal Register, January 6, 2025), and the comment period closed March 7, 2025. As of mid-2026 it is still proposed: no final rule has been issued, and the government’s regulatory agenda now points at roughly 2027 for final action. Treat any vendor claim that these rules are “already law” as a red flag.
Plan for it anyway. The proposed rule would make controls that used to be “addressable” into hard requirements: MFA on every ePHI access path, encryption of ePHI at rest and in transit, documented network segmentation, an asset inventory and network map, vulnerability scanning, and annual technical testing. HHS wrote it in response to a blunt trend — from 2018 to 2023 the number of people affected by large breaches rose 1,002%, and 2023 alone hit a record 167 million. Once a final rule lands, expect it to take effect 60 days after publication with about 180 more days to comply. Teams that wire MFA and encryption in now inherit no scramble later.
Reach for MFA-everywhere when any account can reach ePHI — which is every account. Admin consoles, jump hosts, backup-restore workflows, and service accounts all need it before go-live. The Change Healthcare entry point was a single portal without it.
HIPAA penalty tiers and what enforcement looks like
How much can a HIPAA violation cost? The penalty is tiered by culpability and adjusted for inflation every year. The 2025 amounts run from $145 per violation at the low end to $2,190,294 as the annual cap per identical provision. The table below shows the current tiers; the point is the top row, where willful neglect left uncorrected turns a single systemic failure into a seven-figure liability.
| Tier | Culpability | Per violation (2025) | Annual cap |
|---|---|---|---|
| Tier 1 | No knowledge | $145 – $73,011 | $2,190,294 |
| Tier 2 | Reasonable cause | $1,461 – $73,011 | $2,190,294 |
| Tier 3 | Willful neglect, corrected in 30 days | $14,602 – $73,011 | $2,190,294 |
| Tier 4 | Willful neglect, uncorrected | $73,011 – $2,190,294 | $2,190,294 |
In practice, OCR’s 2019 enforcement discretion caps the lower three tiers well below that ceiling; only willful neglect left uncorrected reaches the full $2,190,294. The fine is rarely the whole bill. OCR settlements now routinely bundle a 2–3 year Corrective Action Plan with an external monitor, and post-Change-Healthcare the agency opened more investigations than in any prior year. The monitoring cost usually dwarfs the penalty. Enforcement is real, and it lands hardest on teams that cannot produce evidence when asked.
Lessons from the Change Healthcare breach
The BlackCat/ALPHV attack on Change Healthcare in February 2024 is the most instructive incident in modern US healthcare software. UnitedHealth’s final count, reported to OCR in July 2025, was 192.7 million individuals. Claims processing froze for weeks across the country. Three root-cause lessons the industry absorbed fast are worth stealing.
One: MFA gaps are the whole ballgame. The entry vector was a remote-access portal without multi-factor authentication. Two: backups are a security concern, not an ops footnote. Backups that are not network-segmented from production get encrypted along with everything else. Three: vendor concentration is systemic risk. A large share of US claims flowed through one processor, and its outage became everyone’s outage. Regulators are now pushing for architectural redundancy in clearinghouses and similar hubs.
Reach for immutable, offline, tested backups when you store any ePHI. That means immutable storage (S3 Object Lock, Azure Immutable Blob), a network-segmented restore environment, and a quarterly restore drill you actually run. A backup you have never restored is a guess, not a control.
Shipping a HIPAA or GDPR product?
We have built telemedicine, imaging, and clinical tools under HIPAA and GDPR for over a decade.
Send us your architecture and regulatory footprint. We’ll come back with a fixed-price compliance plan inside two business days.
GDPR Article 9 and the Schrems II transfer problem
GDPR Article 9 treats health, genetic, and biometric data as special-category personal data. The default is that processing is prohibited unless one of ten exceptions applies. For healthcare software the two that matter are processing “necessary for medical diagnosis or the provision of healthcare” under Article 9(2)(h), which requires an EU or member-state legal basis or a contract with a health professional, or explicit, documented consent.
The harder problem is moving that data across borders. Schrems II invalidated Privacy Shield and made EU-to-US transfers of health data genuinely hard. The durable mechanism today is Standard Contractual Clauses plus supplementary technical measures: encryption keys held inside the EU, so the US cloud vendor cannot produce readable data even under a lawful US government request. The 2023 EU-US Data Privacy Framework offers another route, but its long-term durability is not guaranteed, so betting the architecture on it is risky. EU-region residency for the primary database is effectively mandatory for any serious EU-facing health product.
HITRUST vs SOC 2 vs ISO 27001: when each matters
Which certification should you chase first? It depends entirely on who is buying. SOC 2 Type II is the floor for any B2B healthcare SaaS. HITRUST is what large hospital systems increasingly demand. ISO 27001 is the globally recognized governance baseline. They overlap heavily, so the order you pursue them in is a budgeting decision, not a technical one.
| Framework | What it signals | Pursue when |
|---|---|---|
| HITRUST CSF (e1/i1/r2) | Healthcare-specific; rolls up HIPAA, NIST, ISO 27001, GDPR | Selling into hospital networks, payers, or large health systems |
| SOC 2 Type II | Operating-effectiveness attestation on five trust criteria | Table stakes for any B2B SaaS in US healthcare |
| ISO 27001 | Generic ISMS certification, recognized worldwide | International footprint or a governance baseline |
A workable sequence for a digital-health startup: SOC 2 Type II in year one, ISO 27001 in year two if you go international, HITRUST r2 in year three once enterprise hospital buyers dominate the pipeline. A HITRUST r2 certification already covers most SOC 2 controls and much of ISO 27001, so the incremental cost past it is real but not brutal.
FDA SaMD, PCCP, and the QMSR and EU MDR timelines
Is your software a medical device? If it diagnoses, treats, or mitigates disease, it is Software as a Medical Device and falls under FDA oversight. The fastest way to answer for your own product is to walk the questions in Figure 2.
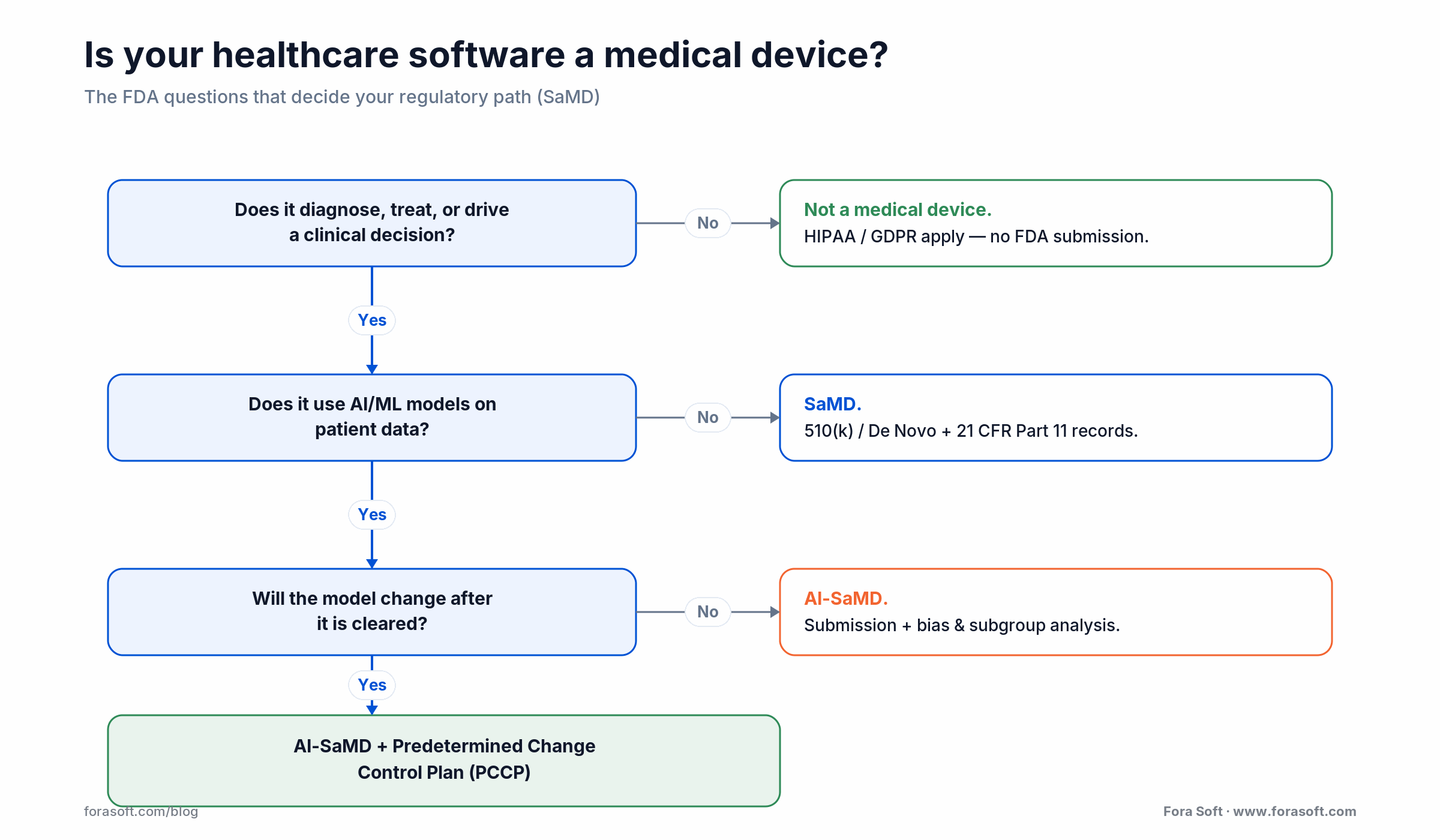
Figure 2. The FDA questions that decide whether your software is a medical device, and which pathway applies.
Two 2026 dates matter for device makers. The FDA Quality Management System Regulation (QMSR, 21 CFR Part 820), which folds ISO 13485:2016 into US device rules, became mandatory on February 2, 2026. EUDAMED became mandatory for new EU registrations on May 28, 2026 across four of its six modules, with legacy devices due by November 28, 2026. EU Notified Body review still averages 13–18 months and runs longer for AI-enabled devices.
| Milestone | Date | What changes |
|---|---|---|
| FDA PCCP final guidance | Dec 4, 2024 | How to pre-authorize model updates for AI devices |
| FDA AI lifecycle guidance (draft) | Jan 7, 2025 | Bias analysis, transparency, lifecycle expectations |
| FDA QMSR mandatory | Feb 2, 2026 | ISO 13485:2016 incorporated; replaces the old QSR |
| EUDAMED mandatory (new devices) | May 28, 2026 | Registration required across four EUDAMED modules |
21 CFR Part 11 applies separately whenever the software creates electronic records or signatures the FDA relies on. It demands validated systems, per-action audit trails, access controls, and signature metadata (name, timestamp, meaning). Part 11 validation is engineering work, not paperwork: a traceability matrix mapping every requirement to a test case, automated regression on those tests, and documented change control.
Encryption: AES-256, TLS 1.3, and key management
AES-256 is the at-rest standard. TLS 1.3 is the in-transit standard; TLS 1.2 is grudgingly accepted, and TLS 1.0 and 1.1 will fail a penetration test. Keys live in a dedicated KMS — AWS KMS, Azure Key Vault, GCP Cloud KMS, or HashiCorp Vault. The non-negotiables: application servers never see raw key material, data-encryption keys are wrapped by key-encryption keys in an HSM, keys rotate on a schedule, and every key access is logged and alertable.
For a dual-region HIPAA plus GDPR deployment we hold customer-managed keys in the EU region for EU patients and separate keys in the US region for US patients. The application uses a tenant-to-region map to decide which KMS to call. That keeps the cryptographic boundary legible to an auditor and makes Schrems II compliance demonstrable rather than hand-waved. We layer the same pattern under AI features through our AI integration services.
MFA, SSO, SMART on FHIR, and OAuth 2.0
MFA is the baseline, including for admin accounts and service accounts. Prefer phishing-resistant methods: NIST SP 800-63B classes SMS as a “restricted” authenticator, so every admin account should use a passkey or hardware token, not an SMS code. For service accounts, issue short-lived OIDC tokens through a workload-identity provider instead of static credentials. SSO via SAML 2.0 or OIDC is expected by any customer above 100 seats.
For EHR integration, SMART on FHIR sits on top of OAuth 2.0 and OpenID Connect: the app registers with the EHR, the user consents to scopes, and the app gets a token limited to specific FHIR resources. Here is the catch worth knowing early — SMART on FHIR does not enforce HIPAA audit logging or session timeout. Those belong to your IAM platform (Okta, Ping, Keycloak) and your own application events. Do not assume the EHR integration covers your audit trail.
Reach for SMART on FHIR when you need to read or write data inside a hospital’s existing EHR (Epic, Cerner) with scoped, consented access. Reach for a plain OAuth 2.0 plus your own IAM when the data lives in your product and no EHR is in the loop.
Audit logging: six-year retention and what to log
HIPAA requires six years of retention for audit logs, policies, and procedures; some states push that to seven or ten. Log every access to ePHI: reads, writes, and deletes on a patient record, bulk exports, and any API call that returns ePHI. Log authentication events, both success and failure. Log authorization changes such as role grants. Log administrative actions like schema changes and infrastructure edits that touch the ePHI boundary.
Instrument end to end. OCR has cited entities for having application logs but no database-layer logs, and the reverse. The pattern that holds up: the application emits structured JSON events, infrastructure logs ship to the same SIEM, the SIEM writes to an immutable tier with customer-managed keys, and retention runs on automated lifecycle rules. Keep that storage in a separate, security-team-controlled account so the logs stay out of reach when the primary environment is compromised.
Telemedicine compliance: state licensing and DEA rules
Telemedicine is a hard regulatory case because compliance follows the patient’s location, not the provider’s. A physician in Texas treating a patient sitting in New York needs a New York license. The Interstate Medical Licensure Compact streamlines this across 44 states (plus DC and Guam) as of 2026, but your software still has to know, at visit time, where the patient is and refuse to connect if the provider is not licensed there.
Controlled-substance rules add a second layer. DEA and HHS extended the telemedicine prescribing flexibilities through December 31, 2026 (the fourth temporary extension), letting providers prescribe Schedule II–V without a prior in-person visit, with audio-only allowed for buprenorphine in opioid-use-disorder treatment. A permanent Special Registration framework is still in rulemaking. Build telemedicine platforms to integrate state PDMPs at prescription time and to gate controlled-substance flows behind an auditable verification step.
Fora Soft field note — CirrusMED
We built CirrusMED, a Direct Primary Care telehealth platform, from scratch for a Nevada practice: unlimited video visits, 24/7 messaging, prescription management, and an EMR in one HIPAA-compliant, browser-based system. It now serves patients across 48+ US states. The state-licensing rule above is not theory for us — the platform checks provider license, patient geolocation, and controlled-substance flags at the start of every session, because catching an edge case after the visit starts means refunding a visit and logging an incident.
AI/ML in healthcare software: the FDA guidance
The FDA has moved from signals to specifics on AI. Its Predetermined Change Control Plan guidance was finalized on December 4, 2024, and a broader draft on AI-enabled device software followed on January 7, 2025. Together they set three expectations for any AI-enabled SaMD. First, bias analysis: validate performance on demographically diverse external data and document subgroup results by age, sex, race, and comorbidity. Second, explainability pitched at the intended user, since a physician and a patient need different depths. Third, a Predetermined Change Control Plan that specifies which model updates you can ship without a new submission.
Foundation models and LLMs get explicit mention: the FDA expects input validation and output verification around any LLM component. In practice a clinical-facing LLM feature needs a deterministic guardrail layer — rule checks, forbidden-phrase filters, citation validators — and a documented human-override flow. That validation discipline is the same one we describe in how we test AI models before they reach production.
Reference architecture for a HIPAA + GDPR dual stack
Our default dual-region reference architecture is deliberately opinionated. One VPC per region, one managed database per region with customer-managed keys held in that region, a tenant router at the edge, and a shared control plane for deployments and monitoring that never touches ePHI. EU-tenant traffic terminates only in the EU region; US-tenant traffic only in the US. Cross-region replication of ePHI tables is absent by design; only non-ePHI metadata like feature flags replicates. Figure 3 shows the shape.
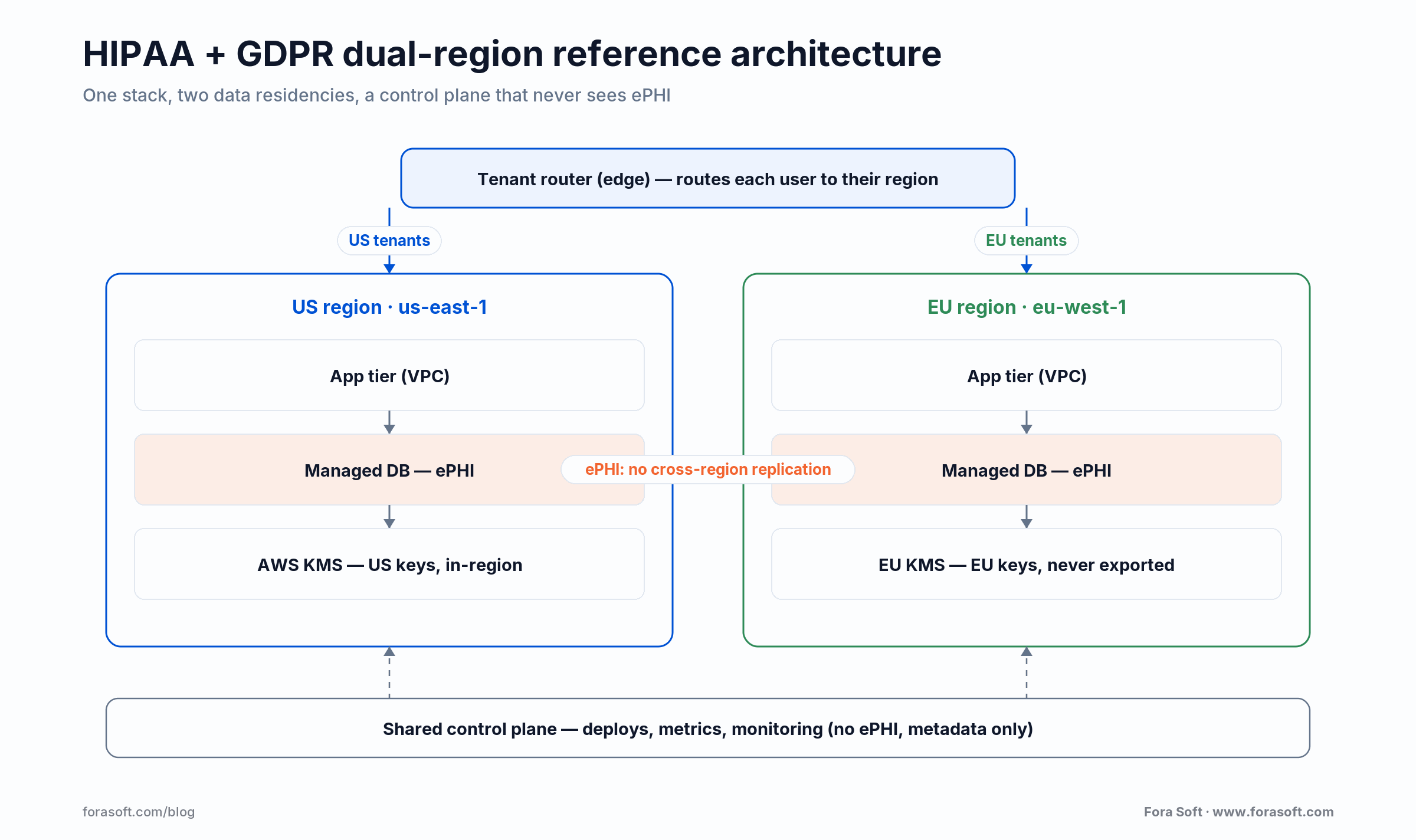
Figure 3. A dual-region HIPAA + GDPR stack: per-region keys, no cross-region ePHI replication, a control plane that never sees ePHI.
Data-science and support access runs through a just-in-time elevation workflow (Teleport or AWS Session Manager) with no standing admin; every elevation is logged, justified, and reviewed. Penetration tests run at least quarterly, and DAST runs on every pull request. The pattern costs a little more than a single-region stack, and it holds up under OCR, the ICO, and a Fortune-500 hospital security review.
Skip the 18-month compliance detour
Our reference stack starts HIPAA, GDPR, and SOC 2 compliant on day one.
Tell us your regulatory footprint and feature scope. We’ll send an end-to-end delivery plan, compliance included, inside two business days.
Secure SDLC: build compliance into every phase
Compliance-as-an-afterthought is the most expensive bug in healthcare software. Bake it into every phase instead. In discovery, identify the regulatory footprint and threat-model the data flows. In design, draw the ePHI boundary explicitly, require KMS-backed encryption for every store, and define the audit events. In implementation, run SAST, secrets scanning, and dependency checks on every pull request. In testing, add DAST, authenticated scans, and PII scanners on test data. In deployment, review infrastructure-as-code for open security groups and unencrypted volumes. In operations, run a SIEM, runtime threat detection, and quarterly tabletop exercises.
Reach for compliance-in-CI/CD when you want features to ship faster, not slower. Teams that pre-audit every merge reach staging clean; teams that treat compliance as a release gate rework 10–20% of the codebase before every major audit.
What healthcare software compliance costs
How much does compliance cost? Split the answer in two. The first cost is the compliance program itself — risk assessment, tooling, training, and audits — which scales with company size, shown in Figure 4. The second is the engineering premium of building compliant software, which is separate and easy to underestimate.
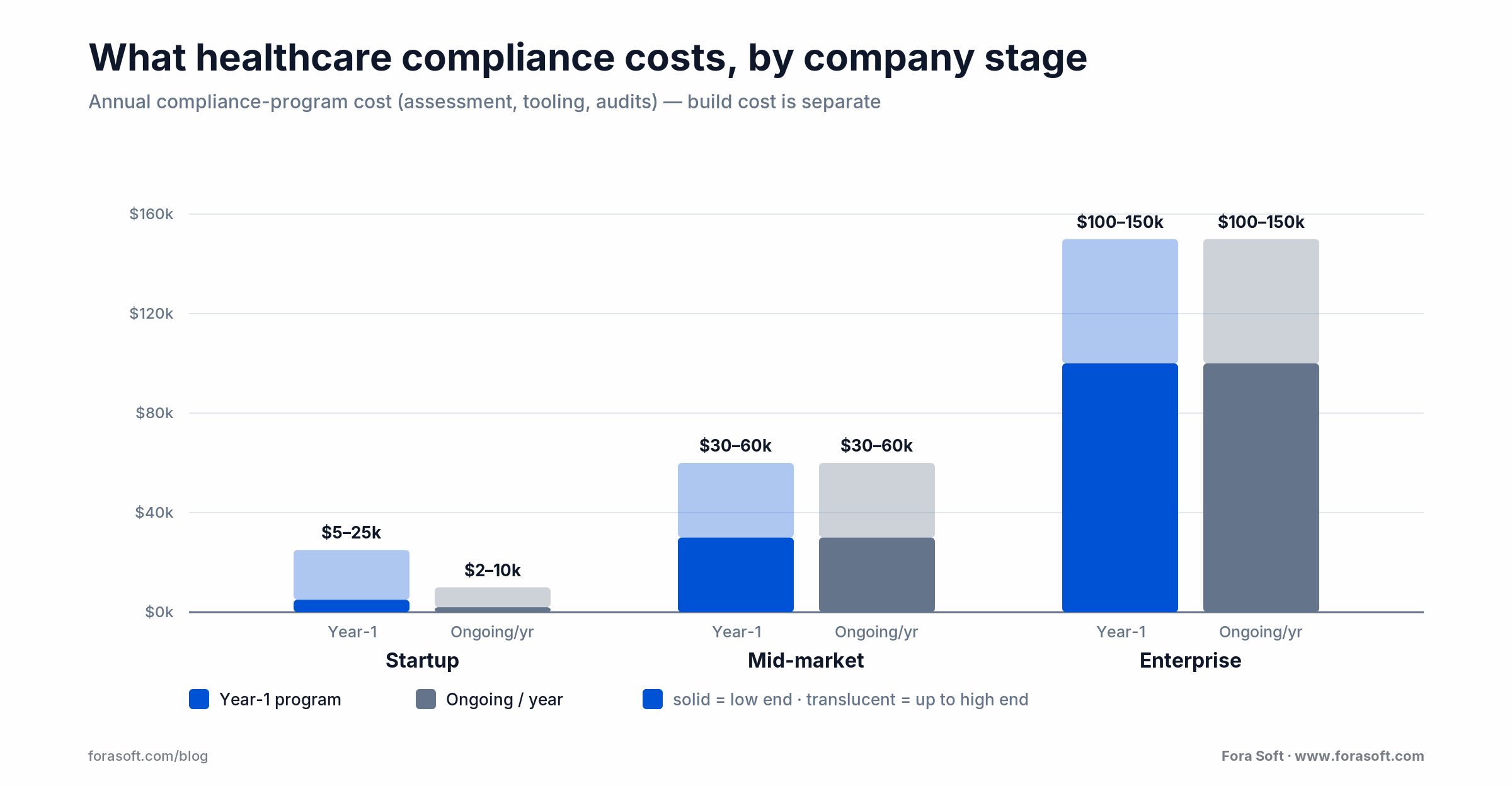
Figure 4. Typical annual compliance-program cost by company stage. The build premium is separate; see the worked math below.
| Stage | Year-1 program (USD) | Ongoing annual |
|---|---|---|
| Early-stage digital-health startup | $5k – $25k | $2k – $10k |
| Mid-market (100–500 employees) | $30k – $60k | $30k – $60k |
| Enterprise (1,000+ employees) | $100k – $150k+ | $100k – $150k+ |
Now the build premium, with the arithmetic shown. A net-new HIPAA plus SOC 2 product typically carries a 15–25% engineering premium over an unregulated equivalent. On a $400,000 base build that is $400,000 × 0.15 to 0.25, or $60,000 to $100,000 of extra work: dual-region key management, audit instrumentation, access controls, and the evidence trail an auditor asks for. We use Agent Engineering to compress the base build, so that percentage lands on a smaller number than a traditional shop would quote. When a figure is genuinely uncertain, we would rather not publish it than inflate it.
Vendor risk: BAAs, sub-processors, and the transitive problem
Every vendor that touches ePHI needs a signed Business Associate Agreement. That rule is easy. The hard part is transitive: your vendor’s vendor also needs a BAA with your vendor, and so on down the chain. A cloud KMS, a monitoring tool, an email service — if any of them passes ePHI without a BAA, your posture breaks the moment a regulator asks the second-order question.
Keep a vendor register with BAA status, sub-processor disclosures, and last-reviewed date. Re-review on every renewal and whenever a vendor publishes new sub-processors. For anything shipping to the EU, document the transfer mechanism (SCCs) and the supplementary technical measures. The paperwork is dull and it is the difference between a clean audit and a seven-figure finding.
When not to build custom healthcare software
Custom is not always the right call, and saying so builds more trust than pretending otherwise. If your need is a standard EHR, scheduling, or billing workflow that an established platform already covers under a BAA, buy it — you will not out-compliance Epic or athenahealth on undifferentiated plumbing. If you have no clinical or product differentiator, a configured SaaS gets you to market faster and cheaper.
Build custom when the differentiator is the software: a novel care model, a proprietary AI feature, an integration no vendor offers, or a data-residency and control posture off-the-shelf tools cannot meet. That is where a HIPAA-fluent telemedicine and healthcare team earns its fee. If you are unsure which camp you are in, that itself is worth a 30-minute conversation before you commit a budget.
How Fora Soft builds compliant healthcare software
Fora Soft has built software since 2005 — 250+ projects, 50 in-house engineers — and healthcare has been part of that from telemedicine (CirrusMED) to clinical imaging and AR/VR surgical training. Our internal playbook is short and opinionated. Dual-region from day one if the EU is in scope. KMS-backed encryption on every store. MFA everywhere, no exception for admins. Audit logs to immutable, detached storage. Automated security scanning on every pull request. Quarterly pentest, annual external HIPAA risk assessment, SOC 2 Type II by month 12, HITRUST by month 24 when hospital systems are the target.
Two early decisions save the most pain: keep ePHI out of non-production environments (synthetic or anonymized data only in dev, QA, and staging), and design the audit log so a compliance auditor can query it without an engineer — a read-only dashboard or report export. Auditor-friendly logs turn a two-week audit into a one-day one. For a sense of how we scope and price this as a fixed engagement, see our guide to software estimating, and the Video for Telemedicine course for the real-time build details.
Build it compliant the first time
We wire HIPAA, GDPR, and SOC 2 into every healthcare product by default.
Send your regulatory footprint and feature scope. You’ll get an architecture plan and a fixed-price estimate, not a sales deck.
FAQ
What does healthcare software development actually include?
Healthcare software development means building products that handle patient data or clinical workflows — telemedicine, EHR integrations, patient portals, medical imaging, and clinical decision tools — under regulatory constraints. The work spans HIPAA and GDPR security controls, and, when the software makes clinical decisions, FDA SaMD validation. The compliance and security layer is what separates it from general software development.
How long does HIPAA compliance take from scratch?
For a new product with experienced engineers, 3–4 months to reach a documented, audit-ready state. Add 1–2 months for the first external audit if this is your first program. Starting HIPAA-by-default in sprint one is far cheaper than retrofitting later.
Is the new HIPAA Security Rule in effect yet?
No. The 2024 Security Rule NPRM is still proposed as of mid-2026; HHS has not issued a final rule, and final action is now expected around 2027. Its likely core requirements — mandatory MFA and encryption of ePHI — are already best practice, so build for them now rather than waiting.
Do we need HITRUST if we already have SOC 2 Type II?
It depends on the buyer. Small and mid-size healthcare customers usually accept SOC 2. Large hospital systems and health plans increasingly require HITRUST r2. If enterprise hospital contracts are on your 18-month roadmap, start HITRUST prep now — the assessment alone runs 9–12 months.
Can we use LLMs for clinical features without an FDA submission?
Only if the feature is non-diagnostic and non-therapeutic — documentation help, summarization, workflow automation. Once the AI output influences a clinical decision such as diagnosis, treatment, or triage, you are in SaMD territory and need the FDA pathway. Your BAA with the model provider also has to be in place.
How do we transfer ePHI between the EU and US?
Default: don’t. Keep EU patient data in-region. If transfer is truly necessary, use Standard Contractual Clauses plus encryption keys held in the EU and never exported, so the US provider cannot decrypt on a US government request. Document the mechanism and the supplementary measures in your data protection impact assessment.
What is the minimum MFA we should require?
TOTP from an authenticator app is the floor; WebAuthn or passkeys are better. SMS-based MFA is discouraged under current NIST guidance. Every admin account should require a hardware token or passkey rather than an authenticator app.
How much does it cost to build HIPAA-compliant software?
Separate two numbers. The compliance program runs $5k–$25k in year one for a startup and $100k+ for an enterprise. On top of that, building compliant software adds roughly a 15–25% engineering premium over an unregulated equivalent — about $60k–$100k on a $400k build. We use Agent Engineering to shrink the base, so the premium applies to a smaller total.
What to read next
Telemedicine
Telehealth software development
The feature set and compliance concerns behind a modern telehealth build.
Healthcare
Nurse call systems: build vs buy and HIPAA
A build-vs-buy playbook for HIPAA-grade clinical communication.
Architecture
AI in software architecture design
Where AI models fit inside regulated architectures like healthcare.
Quality
AI testing and validation
Validation strategies for AI features before they reach clinical users.
Estimating
Guide to software estimating
How we estimate a HIPAA-compliant delivery as a fixed-price engagement.
Ready to build compliant healthcare software?
Fora Soft has shipped HIPAA, GDPR, and SOC 2 software across telemedicine, clinical imaging, and clinical decision support for over a decade. We architect for compliance from day one and send you a fixed-price delivery plan inside two business days.
Start a compliant build
Book a 30-minute call with Fora Soft
Send us your regulatory footprint, scope, and timeline. We’ll reply with an architecture plan and a fixed-price estimate.








