


Key takeaways
• A telesitter turns one-to-one watching into one-to-many. Instead of a paid sitter in every at-risk patient’s room, one trained observer watches a wall of video feeds and talks to patients through two-way audio. Health systems commonly run one observer to twelve patients, sometimes up to sixteen.
• The business case is falls and sitter labor, not gadgets. In-hospital falls are a non-reimbursable “never event,” and 1:1 sitters cost some hospitals over a million dollars a year. Independent, peer-reviewed evidence shows virtual sitting usually cuts falls and reliably cuts sitter cost.
• The hard engineering is escalation and privacy, not the video. An observer can only speak and phone for help — so the alert path to a bedside nurse, and the privacy design that keeps a patient’s room from becoming a data-leak, are what make or break the product.
• Every serious vendor is quote-only. AvaSure, Caregility, Teladoc, Equum, Hicuity, and Collette Health all price per deployment, and a single AvaSure device has shown up in a federal solicitation near $53,000. That opacity is a big reason health systems ask whether to build.
• Buy the platform when you want it running this quarter; build when it’s strategic. A custom telesitter platform wins when you need EHR-deep integration on your terms, data residency a vendor cloud can’t give you, or a system that fits a workflow no product sells. Otherwise, buy.
At 3 a.m. on a medical-surgical floor, a confused post-op patient decides to walk to the bathroom alone. A year ago the only defense was a $21-an-hour sitter parked in a chair by the bed — if one was free that night. Today, a monitor tech two floors away sees the patient reach for the rail, says “Please wait, someone is coming” through the room speaker, and taps a button that rings the charge nurse’s phone. The patient stays in bed. That swap — a chair in every room for one screen watching many — is what a telesitter platform is, and why virtual patient observation has become one of the fastest-moving line items in hospital operations.
We’ve built real-time video and computer-vision systems since 2005, including large-scale video surveillance platforms and live incident-detection pipelines. So this is an engineer’s guide, not a brochure: what a telesitter actually is, how virtual patient observation works, what the independent evidence says, how the platform is built, what it costs, how the vendors compare, and when a hospital is better off building its own instead of buying one.
Weighing a telesitter platform?
Tell us your setting — a single unit, a hospital, or a multi-site system — and we’ll give you a straight read on whether to buy a platform or build one, with the integration, privacy, and cost tradeoffs behind the call.
Why Fora Soft wrote this guide
We’re a video and AI software company: 250+ projects since 2005 and a team of about 50 engineers. A large share of that work is exactly the plumbing a telesitter platform needs — capturing many live video streams at once, running computer-vision models on them in real time, moving low-latency two-way audio into a room, and routing an alert to the right human fast enough to matter. When someone asks us to watch dozens of feeds and act on an event within seconds, we’ve usually built the underlying pieces already.
One example is VALT, a HIPAA-grade video observation and recording platform we’ve been the sole development team for over a decade — now used by 770+ US organizations and 50,000+ users. It is multi-camera observation infrastructure with privacy controls and audit trails, which is the same backbone a hospital telesitter system runs on. We’ve also built real-time incident detection on live video, the kind of motion-and-event alerting a telesitter platform layers on top.
We don’t operate a telesitter monitoring service — we don’t staff the observers or sell a boxed product — so there’s nothing to push here. For many hospitals, buying a mature platform is the right answer, and we’ll say so. What we build is the custom version, which means we’ve earned the right to be honest about when you don’t need one.
What a telesitter is (and what “virtual patient observation” means)
A telesitter is remote, continuous video-and-audio observation of at-risk patients, where one trained observer watches several patients at once and intervenes by speaking to them through two-way audio, escalating to the bedside nurse when someone needs hands-on help. “Virtual sitter,” “virtual patient observation,” and “remote patient observation” are the same idea under different names; “telesitter” is the term that stuck, partly because AvaSure trademarked it after introducing the category in 2008 (AvaSure, 2026).
The job it replaces is the “1:1 sitter” or “patient safety attendant” — a staff member assigned to stay within arm’s reach of one patient who might fall, pull out a line, or wander. That role is expensive and hard to fill. A telesitter keeps the same protective idea — a set of eyes that never leaves — but points it at many rooms through cameras instead of one room through a chair.
It helps to be precise about what a telesitter is not. It is not a nurse call system, which waits for the patient to press a button. It is not general hospital video surveillance, which records corridors for security. And it is not remote patient monitoring: RPM tracks vitals through devices the patient wears or uses, while a telesitter watches behavior in the room and needs nothing on the body at all. The two are complementary — one knows the heart rate, the other sees the patient trying to climb out of bed.
One more distinction shapes the whole design: a telesitter observer intervenes with words, not hands. They can redirect a patient (“please stay in bed, help is on the way”), and they can summon staff. They cannot physically catch anyone. Everything hard about building the platform flows from that fact — the value lives in how fast and reliably the system turns something seen into someone arriving.
The short answer: buy a platform, buy a service, or build
Buy a platform (AvaSure, Caregility, and peers) if you run one or a few hospitals and want proven virtual observation with the hardware, monitoring software, and clinical workflows handled for you. You get a system deployed in months rather than a build, at a per-deployment price you’ll have to request — and for most health systems this is the right call.
Buy a managed service (Equum Medical, Hicuity Health) if you want the outcome, not the operation: the vendor staffs the observers from their own monitoring center and bills you for coverage. It shifts the labor of running a 24/7 hub off your books, which is attractive if your bottleneck is people, not technology.
Build a custom platform when virtual observation is strategic rather than a purchase — when you need it woven deep into your own EHR and nurse-call workflow, when data-residency or security rules keep video off a vendor’s cloud, when you’re a health-tech company shipping observation as your own product, or when subscription costs at your scale have outgrown a one-time build. The rest of this guide is the evidence behind those three paragraphs.
How virtual patient observation actually works
The loop is short: a nurse enrolls an at-risk patient, a camera in the room streams to a central hub, an observer watches a grid of patients, and when someone starts to do something unsafe the observer talks them down and, if needed, escalates to the floor. Everything else is detail in service of making that loop fast and trustworthy.
Enrollment. A patient becomes a candidate through a clinical order — typically placed right in the EHR. At St. Luke’s in Duluth, an RN orders virtual observation in Meditech Expanse, which notifies the monitor specialists (Healthcare IT News, 2024). Not everyone qualifies: Johns Hopkins keeps an in-person sitter for the first two hours and reverts to 1:1 if a patient is pulling at lines (Johns Hopkins, 2019).
Observation. A pan-tilt-zoom camera unit — on a mobile pole, mounted to the ceiling, or built into the room — streams live video and audio to a monitoring station. One observer watches a tiled grid, adjusting a camera to keep a restless patient in frame. Some platforms overlay motion or AI triggers to flag a patient who sits up or swings a leg over the rail, so the observer’s attention is drawn before, not after, the movement.
Intervention and escalation. When a patient starts to get up, the observer speaks through the room speaker to redirect them. If words aren’t enough, the observer escalates — a call or page to the bedside nurse’s phone, often through the same system that placed the order. Speed here is the entire product: the seconds between “observer sees it” and “staff arrives” are what a fall happens inside of.
The economics: why hospitals adopt telesitters
The case for virtual observation rests on two numbers hospitals already feel: the cost of falls and the cost of sitters. Between 700,000 and 1 million patients fall in US hospitals each year, at roughly three to five falls per 1,000 bed-days, and more than a third of those falls cause injury (AHRQ PSNet, 2024). A serious fall in a care facility is classed as a “never event,” and Medicare will not reimburse the hospital for the added cost of treating it — so an injurious fall is both a harm to the patient and a direct hit to the hospital’s margin.
The other number is labor. A 1:1 sitter is a full staff member per at-risk patient, and demand spikes unpredictably. One Tennessee community hospital reported staffing 14 sitters a day at $425,000 a year (Association of Health Care Journalists, 2023), and larger systems routinely cite annual sitter spend in the seven figures. With labor running well over half of hospital costs and rising sharply (American Hospital Association, 2025), a model that turns twelve sitters into one observer is compelling on the spreadsheet alone.
The honest framing: a telesitter doesn’t eliminate sitters — it concentrates them. You still pay observers and still keep some 1:1 coverage for the highest-acuity patients. The saving comes from the ratio, and the ratio only holds if the escalation path is fast enough that watching many patients stays as safe as sitting with one. Design the escalation badly and the “saving” is just risk moved off the budget and onto the patient.
Does it actually work? What the evidence says
Mostly yes on cost, and usually yes on falls — with honest caveats. The most useful independent source is a peer-reviewed literature review that pooled twelve studies: eight showed a reduction in falls, the rest showed no statistically significant change or did not isolate a fall rate, and all twelve reported lower overall cost after moving from 1:1 sitters to virtual observation. The authors flag small sample sizes as the main limitation (Hogan Quigley et al., Computers, Informatics, Nursing, 2021). In other words: the cost savings are well supported; the fall-reduction effect is real but not universal.
Named health-system results back that up. Johns Hopkins Bayview reported saving more than $1 million over one year with its TeleSitter program, with no falls-with-injury during a six-week pilot (Johns Hopkins, 2019). St. Luke’s in Duluth logged over 164,000 observation hours across 16 devices and reported more than $1.5 million saved in 2023, cutting 1:1 sitter use by as much as 73% on some units (Healthcare IT News, 2024). These are single-site operational reports, not controlled trials — strong signal, appropriately hedged.
Read vendor numbers carefully: AvaSure publicly cites figures like 6X ROI, a 75% cut in 1:1 sitter reliance, and customer savings of $10M+ (UC San Diego Health) and $23M (Trinity Health) (AvaSure, vendor page, retrieved 2026-07-16). Those may well be real, but they’re customer results published by the seller, and the same page elsewhere quotes different reduction percentages. Anchor your own business case on the independent review and named health-system reports above, and treat vendor headline stats as the optimistic end of the range.
Anatomy of a telesitter platform
A production telesitter platform is four layers: the camera units in the rooms, a real-time media backbone that carries video and two-way audio, a central monitoring hub where observers work, and an integration layer that ties enrollment and escalation into the EHR and nurse-call systems. Get any one of them wrong and the whole thing feels either unsafe or unusable.
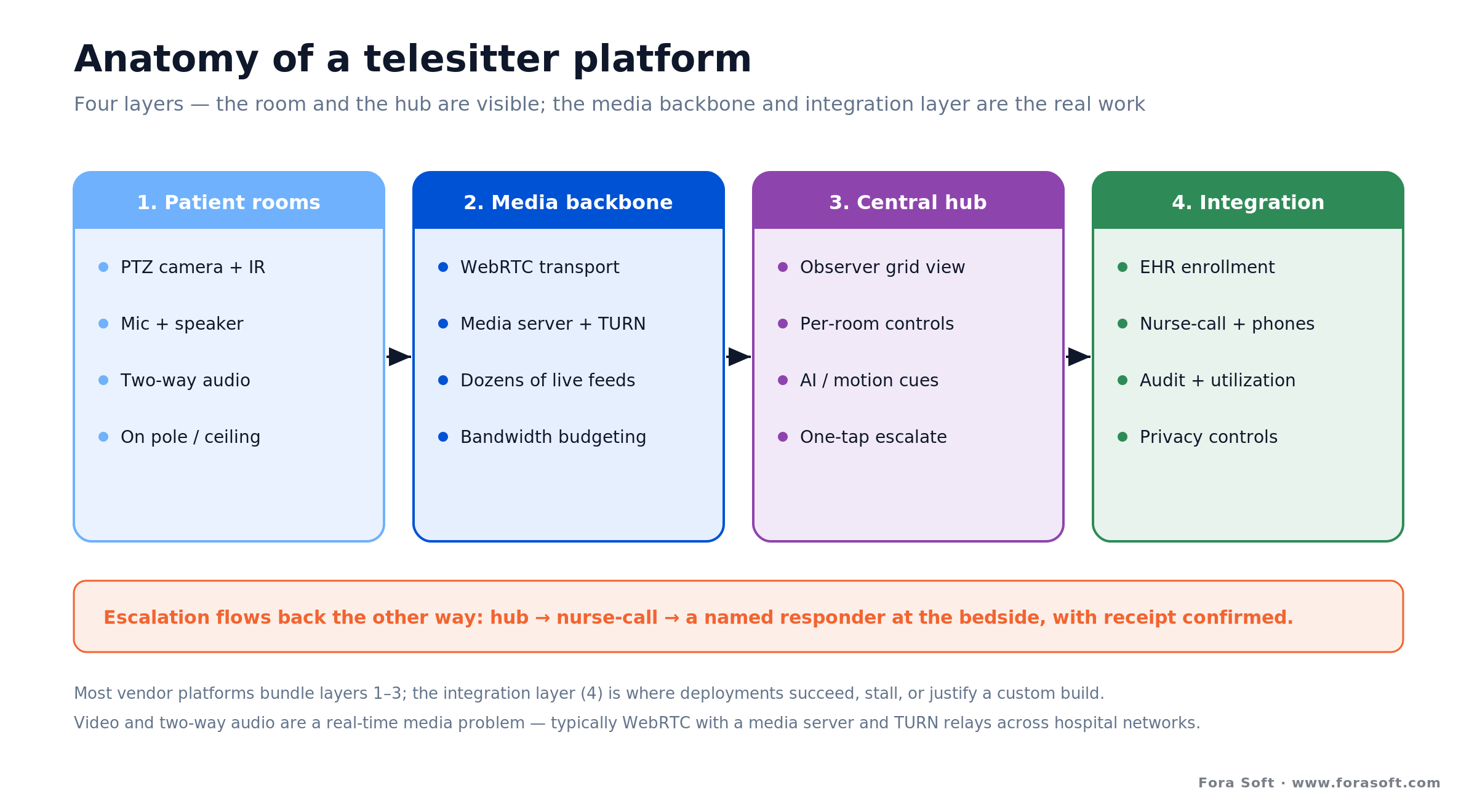
Figure 1. The four layers of a telesitter platform. The room and the hub are the visible parts; the media backbone and the integration layer are where the engineering effort actually goes.
The room. A PTZ camera with strong low-light or infrared performance, a microphone, and a speaker for two-way audio. Commercial units pair a 1080p sensor with 10x–20x zoom and pan/tilt so one observer can keep a moving patient framed (AvaSure devices, 2026; Caregility APS carts, 2026). Mounting matters clinically: a pole-mounted cart is flexible but trip-prone; a ceiling mount is tamper-resistant and out of the way.
The media backbone. This is the part teams underestimate. Carrying dozens of simultaneous low-latency video-plus-audio streams over hospital Wi-Fi, with echo-cancelled talk-back into the room, is a real-time media problem — typically WebRTC with a media server, TURN relays for tricky network segments, and careful bandwidth budgeting so a full hub doesn’t degrade every feed at once.
The hub and the integration layer. The hub is the observer’s workstation: a tiled grid, per-room controls, and a one-tap escalation. The integration layer is what makes it clinical rather than a security desk — enrollment orders flowing in from the EHR, escalations flowing out to nurse-call and staff phones, and usage data flowing back for audit and staffing. AvaSure’s 2026 Epic integration designation exists precisely because this layer is where deployments succeed or stall.
The alert path: from motion to a nurse at the bedside
Because the observer can’t physically intervene, the escalation path is the safety-critical core of the system. It runs from a trigger, through a human decision, to a person arriving in the room — and every step has a failure mode you have to design against.
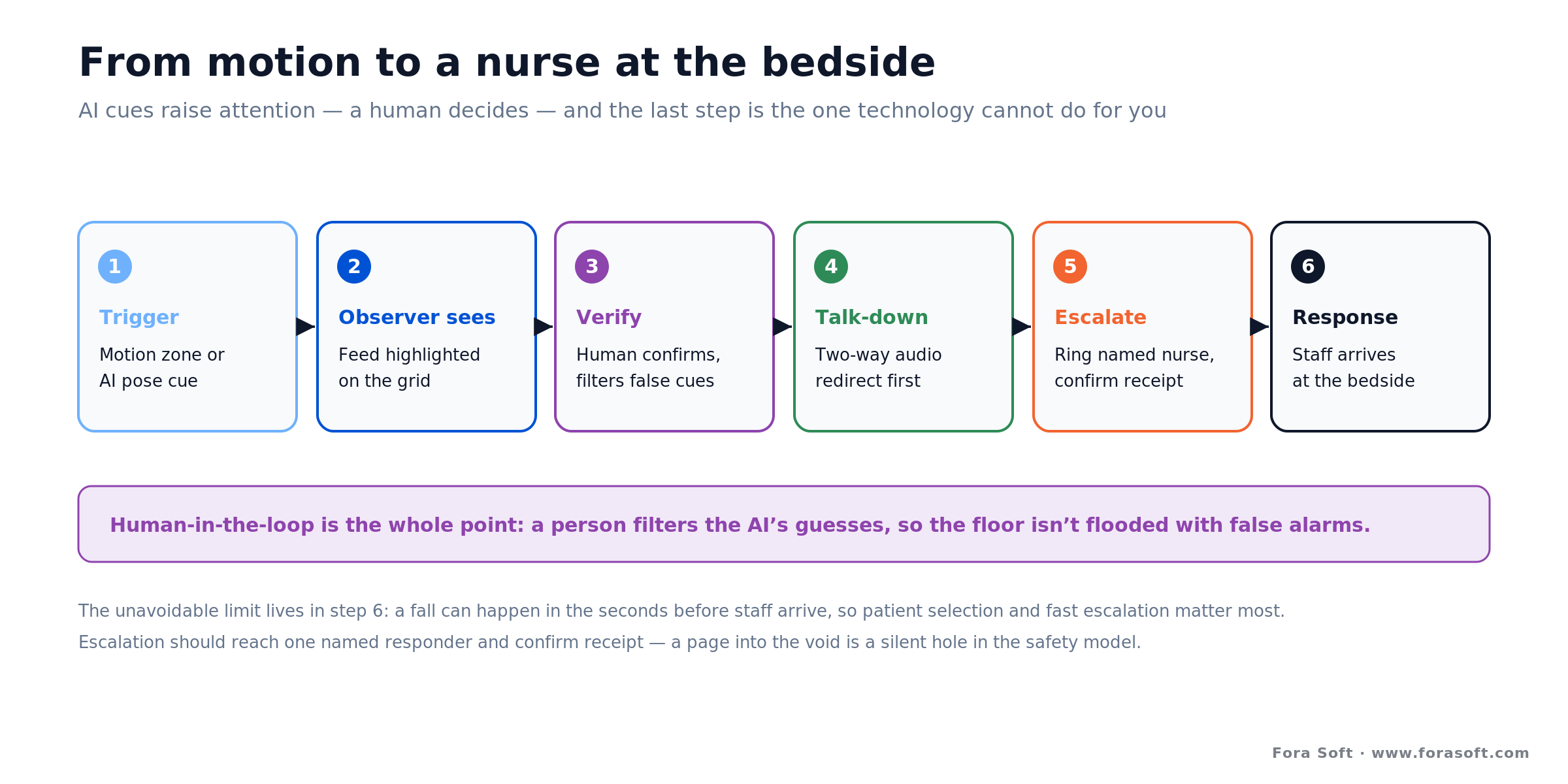
Figure 2. The escalation pipeline. AI and motion cues raise attention, but a human decides — and the last step, a physical response, is the one the technology can’t do for you.
Trigger. A motion zone or a pose/AI model notices a patient sitting up or moving toward the edge of the bed and highlights that feed. This is assistive, not autonomous: it directs a busy observer’s eyes, it doesn’t page anyone on its own. Tuned too sensitively it cries wolf; too loosely it misses the early cue that buys response time.
Observer decision and redirect. The observer confirms what’s happening and speaks to the patient first — often that alone keeps them in bed. This human-in-the-loop step is why telesitter false alarms don’t flood the floor the way a raw automated detector would: a person filters the AI’s guesses before anyone is interrupted.
Escalate and respond. If words aren’t enough, the observer rings the bedside nurse or charge nurse — ideally through an integrated call to a specific phone, not a general alarm. St. Luke’s routes escalations to monitor specialists and staff through Meditech and ASCOM phones (Healthcare IT News, 2024). The unavoidable limitation lives here: a fall can happen in the seconds before staff arrive, which is why patient selection and fast, unambiguous escalation matter more than any camera spec.
Design rule: escalation should be one unmistakable action that reaches a named responder and confirms receipt. A page into the void is worse than useless — the observer needs to know a human accepted the alert, or the safety model has a silent hole in it.
The staffing model: one observer, many rooms
The economics live in the ratio, and the ratio is a clinical judgment, not a hardware limit. Johns Hopkins runs one clinical technician to twelve patients (Johns Hopkins, 2019). St. Luke’s improved staffing from 1:1 toward 1:12, “sometimes as high as 1:16 depending on acuity” (Healthcare IT News, 2024). AvaSure states an observer can watch up to sixteen patients, and Caregility’s iObserver puts up to twelve on one screen (vendor pages, 2026). The right number for a given unit depends on how active and confused the patients are.
Watching sixteen feeds for hours is its own hazard: monitor fatigue is a recognized operational risk. St. Luke’s counters it with a two-person team that rotates at least every four hours (Healthcare IT News, 2024). A well-built platform helps here — AI attention cues, visual and audible flags, and a layout that surfaces the feed that needs attention rather than asking a tired human to scan a wall of identical tiles.
The staffing model is also why “buy the service” is a real option. Running a 24/7 hub means hiring, training, and scheduling observers around the clock — a workforce problem some health systems would rather hand to a managed-service vendor like Equum or Hicuity than solve in-house.
Privacy by design: a camera in a patient’s room
A live camera in a hospital room is one of the most sensitive data sources a health system can create, and the privacy design is not a setting you add later — it is the architecture. The core choices are whether you record at all, how you hide the room during private moments, and how you prove after the fact that the rules were followed.
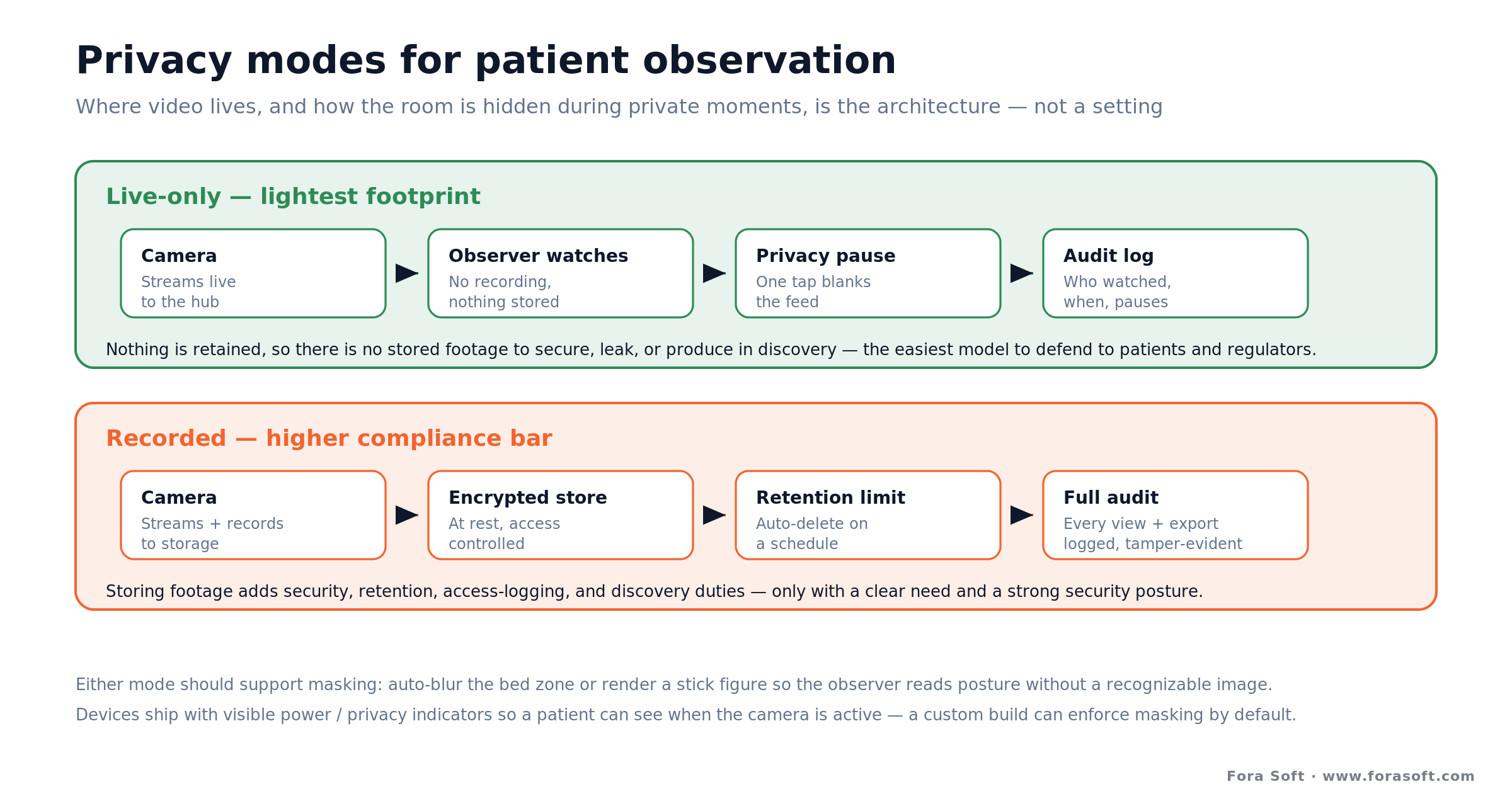
Figure 3. Privacy modes for patient observation. Live-only observation with a manual privacy pause is the lightest-footprint default; recording raises the compliance bar sharply.
Record or not. Live-only observation — watch, never store — is the smallest attack surface and the easiest to defend to patients and regulators. The moment you retain footage, you inherit storage security, retention limits, access logging, and discovery obligations. Many telesitter deployments run live-only for exactly this reason; a build that records needs a much stronger justification and a much stronger security posture, which is where a HIPAA-compliant video platform foundation earns its keep.
Privacy pause and masking. When a clinician performs an exam or a patient uses the bathroom, the observer must be able to blank or blur the feed with one tap, and the system should make that the easy, expected action. Devices ship with privacy modes and visible power/privacy indicators so the patient can see when the camera is active (AvaSure devices, 2026). A custom build can go further — automatic masking of the bed zone, or a stick-figure rendering that conveys posture without a recognizable image.
Audit everything. Who watched which room, when, and when privacy mode was engaged — all of it logged and tamper-evident. This is the same discipline behind secure video communication, and it is what lets a hospital answer “prove the patient’s dignity was protected” with evidence rather than assurances.
HIPAA, consent, and recording
Telesitter video and audio are protected health information the moment they can identify a patient and relate to their care, so HIPAA governs the whole system — the streams, the storage if any, and every account with access. Treat the platform as PHI infrastructure from the first line of code: encryption in transit and at rest, role-based access, minimum-necessary viewing, business-associate agreements with any vendor in the path, and access logs you can actually produce.
Consent is more nuanced than a blanket “HIPAA allows it.” HIPAA generally permits using PHI for treatment and operations without separate written authorization, but many organizations still inform patients and document consent — both for ethics and because some states have two-party consent laws that reach audio recording. If your platform captures or retains audio, that state-law layer needs a lawyer’s eyes, not an engineer’s assumption. We build to the strict interpretation and let counsel relax it, never the other way around.
Where a camera doesn’t belong: some patients and some moments are out of bounds regardless of what the technology can do — behavioral-health situations where surveillance is counter-therapeutic, patients who refuse, and any private-care task without a masking mode engaged. A telesitter should be a documented clinical decision with an opt-out, not a default applied to every bed. The healthiest programs are explicit about that, and the software should make the safe choice the easy one.
Need the privacy and HIPAA layer built right?
We’ve shipped HIPAA-grade video observation used by 770+ organizations. If you’re scoping a telesitter build, we’ll walk you through the record-or-not decision, masking, and audit design before a line of code is written.
The vendors compared: AvaSure, Caregility, Teladoc, and peers
The market splits into platform vendors that sell you the hardware and software to run observation yourself, and managed services that also staff the observers. The single most important thing to know before you shop: none of them publish transparent pricing. Every option below is quote-based, which is exactly why the build-vs-buy question is worth taking seriously.
| Vendor | Model | Pricing (2026-07-16) | Where it fits |
|---|---|---|---|
| AvaSure | Platform (you staff observers) | Quote; ~$53K/device in one federal solicitation | Category leader; Epic integration; broad case library |
| Caregility | Platform (iObserver) | Quote | Up to 12/screen; shares device with tele-consults |
| Teladoc Health | Platform (virtual sitting) | Quote | One device also does virtual nursing and consults |
| Equum Medical | Managed service (vendor staffs) | Quote; cites 50–70% vs 1:1 | You want the outcome, not a 24/7 hub to run |
| Hicuity Health | Managed service (tele-ICU heritage) | Quote; cites 80%+ savings | Systems already using its tele-ICU coverage |
| Collette Health | Platform (AI fall-prediction angle) | Quote | Emphasizes analytics; scale claims across 170+ hospitals |
| Custom build | Your platform, your infrastructure | One-time build + run cost | Deep EHR fit, data residency, or it’s your product |
Vendor claims of “50–70%” or “80%+” savings are self-reported and depend heavily on your baseline sitter spend; use them to frame questions, not to close the business case. The practical takeaway is that comparing options requires a formal quote from each, and once you’re collecting quotes, it costs little to price a build alongside them.
Build vs buy: when a custom platform wins
For a single hospital that just wants fewer falls and lower sitter cost, buying is almost always right — a mature platform is deployed in months and carries clinical validation you don’t have to earn. Building makes sense when one of a few specific conditions is true, and it’s worth being strict about them, because a build you didn’t need is the most expensive way to save money.
Build when: you need observation woven deep into a workflow or EHR configuration no product supports; data-residency, sovereignty, or security rules keep video off a vendor cloud; you’re a health-tech company and observation is part of the product you sell; or you operate at a scale where per-device subscription fees over several years clearly exceed a one-time build plus its run cost.
Buy when: you’re protecting one or a few hospitals, standard clinical workflows fit, you want proven outcomes and vendor support, and you’d rather spend on coverage than on a software team. For most health systems this is the honest answer, and we’ll tell you so before you spend a dollar with us.
There’s also a hybrid worth naming: build the parts that are strategic — the integration layer, the privacy model, the analytics — on top of proven media infrastructure rather than reinventing WebRTC transport from scratch. Most of a telesitter platform’s differentiation is in workflow and compliance, not in moving pixels, so that’s where a custom effort should concentrate.
What a custom telesitter build costs
Two numbers decide a build’s payback: the labor it saves and the labor it still needs. The saving comes from the ratio — replacing many 1:1 sitters with a few observers — and the cost is the platform plus the hub staff you keep. The figure below is illustrative, not a quote, but it shows why the math tends to work even before you count avoided falls.
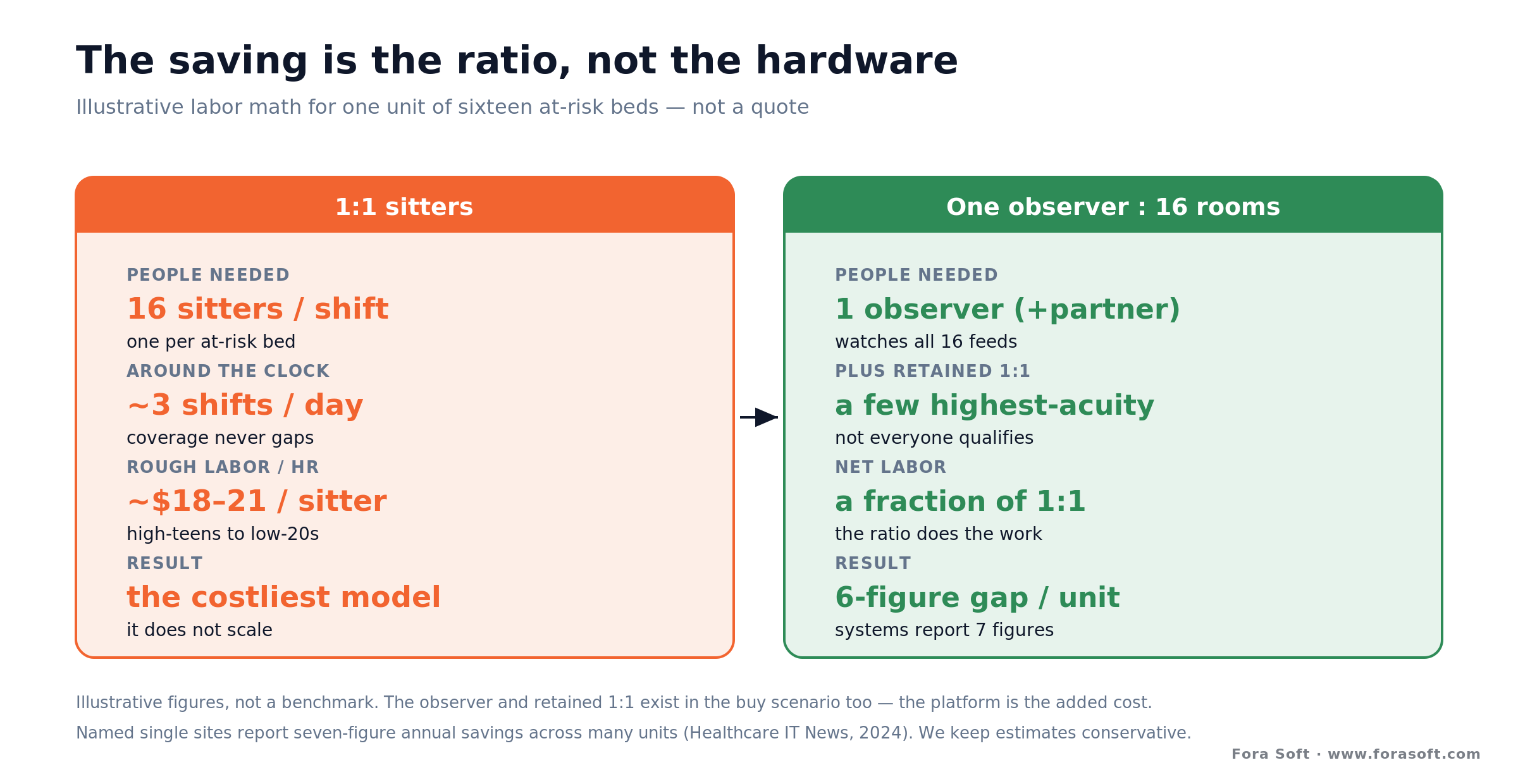
Figure 4. Illustrative labor math for one unit. Covering sixteen at-risk beds with 1:1 sitters versus one observer plus retained safety coverage — the ratio, not the hardware, drives the saving.
The labor swap. Take sixteen at-risk beds. Covering each with a 1:1 sitter around the clock is roughly sixteen times the sitter labor cost. Covering them with one observer per shift — plus a partner to fight monitor fatigue, plus some retained 1:1 for the highest-acuity patients — is a fraction of that. At a sitter cost in the high-teens to low-twenties per hour, the annual gap for one unit runs comfortably into the hundreds of thousands, which is why single sites report seven-figure savings across many units (Healthcare IT News, 2024). We keep these estimates conservative on purpose.
The build cost. A custom platform’s one-time cost is dominated by the media backbone, the observer application, the EHR and nurse-call integration, and the privacy and audit layer — plus hardware per room. Reusing proven real-time infrastructure instead of building transport from scratch is the biggest lever on that number. The recurring cost is cloud or on-prem compute, camera maintenance, and the observers, who exist in the buy scenario too.
The break-even. Because a mature vendor platform is also priced per device with ongoing fees, the build-vs-buy break-even is really software build cost versus years of subscription at your device count. At a handful of rooms, buy. At hundreds of rooms across a system, over a multi-year horizon, a build — or a hybrid — starts to pencil out, and the strategic reasons (integration, data residency, product ownership) often matter more than the raw dollars anyway.
Want the build-vs-buy numbers for your system?
Give us your bed count, current sitter spend, and integration constraints, and we’ll model a build against the vendor quotes you’re gathering — conservatively, with the assumptions on the table.
Mini-case: observation infrastructure at scale
The closest analog in our own work is VALT, a video observation and recording platform we’ve developed as the sole engineering team for more than a decade. It’s used by 770+ US organizations and 50,000+ users, and while its home turf is education and clinical training rather than bedside fall prevention, the backbone is the same one a telesitter platform needs: many cameras, centralized live observation, recording with strict access control, and audit trails that hold up to scrutiny.
What that decade taught us maps directly onto virtual patient observation. Multi-camera live viewing has to stay smooth when a room full of feeds is open at once. Privacy is a first-class feature, not a bolt-on — who can view what, when, and with what record. And the integration surface — making observation fit an institution’s existing systems and roles — is where adoption is won or lost, exactly as it is with EHR integration in a hospital.
On the detection side, our work on real-time monitoring with machine learning and anomaly detection in video surveillance is the same shape of problem as a telesitter’s motion and pose triggers: watch a live scene, surface the moment that matters, and route it to a human without burying them in noise. That’s why, when a health system asks whether a telesitter build is realistic, our answer is grounded in systems we already run.
A telesitter decision framework in five questions
Before you talk to a vendor or a build team, five questions will tell you which path you’re actually on.
1. What’s the scale? A unit or a single hospital points to buying a platform or a service. Hundreds of rooms across a multi-site system, over years, is where a build or hybrid starts to compete on cost alone.
2. How deep does integration need to go? If enrollment and escalation must live inside a specific EHR and nurse-call configuration a product doesn’t support, that pushes toward a custom integration layer — sometimes on top of a bought platform.
3. Where must the video live? If data-residency, sovereignty, or security policy forbids a vendor cloud, your options narrow fast and building your own infrastructure may be the only compliant route.
4. Is this your product or your operation? If you’re a health-tech company selling observation, you build. If you’re a hospital reducing falls, you almost certainly buy.
5. Who runs the hub? If staffing a 24/7 observation center is the hard part, a managed service solves your real bottleneck — and no amount of custom software will.
When NOT to build (or deploy) a telesitter
The technology is genuinely useful, which is exactly why it’s worth being clear about its limits. Don’t build when a mature platform already fits your workflow — you’d be paying to re-earn clinical validation that AvaSure and its peers spent years on. Don’t deploy virtual observation as a blanket substitute for staffing: it concentrates sitters, it doesn’t conjure them, and the highest-acuity patients still need hands in the room.
Be especially careful with the escalation gap. An observer who can only speak and phone for help is not a safety net for a patient who falls in two seconds; virtual observation suits patients you can redirect, not those who need physical restraint of movement. And treat automated fall alerts with humility — a purely automated AI fall detection camera can complement a telesitter, but at facility scale even a very accurate detector generates a stream of false alarms, which is precisely why the human-in-the-loop observer exists.
Finally, don’t deploy where surveillance is clinically wrong — behavioral-health contexts where being watched harms the patient, or any setting where consent can’t be honored. A camera you can’t ethically point at the patient is a camera you shouldn’t install, however good the fall numbers look elsewhere.
FAQ
What is a telesitter?
A telesitter is remote, continuous video-and-audio observation of at-risk hospital patients. One trained observer watches several patients at once on a monitoring screen, speaks to them through two-way audio to keep them safe, and escalates to the bedside nurse when someone needs hands-on help. It replaces the traditional in-room 1:1 “sitter” with a one-to-many model.
What does a telesitter do in a hospital?
A telesitter observer monitors enrolled patients for unsafe behavior — getting out of bed unassisted, pulling at lines, wandering — and intervenes verbally through the room speaker first. If speaking isn’t enough, they alert the bedside or charge nurse to respond in person. The observer watches and communicates; they don’t provide hands-on care.
How many patients can one telesitter observe at once?
Commonly around twelve, and up to sixteen depending on patient acuity. Johns Hopkins runs one technician to twelve patients (2019); St. Luke’s reports 1:12 rising to 1:16 (2024); AvaSure states up to sixteen and Caregility up to twelve per screen. The right ratio is a clinical judgment, not a hardware limit, and busy or confused patients lower it.
Do telesitters actually reduce falls?
Usually, and they reliably cut cost. A peer-reviewed review of twelve studies found eight showed a fall reduction, the rest showed no significant change or did not isolate falls, and all twelve reported lower cost after moving from 1:1 sitters to virtual observation (Computers, Informatics, Nursing, 2021). Named health systems report seven-figure annual savings. The cost benefit is well supported; the fall-reduction effect is real but not universal.
How much does a telesitter system cost?
Every major vendor prices by quote, not a public list. A single AvaSure device appeared near $53,000 in one US federal solicitation (bundling hardware, software, support, and training), and one peer-reviewed study cited a roughly $120,000-per-year program cost offset by savings. Managed services bill for coverage instead of hardware. Because pricing is opaque and per-device, comparing quotes — and pricing a build alongside them — is worthwhile.
Is telesitter monitoring HIPAA compliant?
It can be, and it must be, because the video and audio are protected health information. That means encryption in transit and at rest, role-based access, minimum-necessary viewing, business-associate agreements with any vendor in the data path, and access logging. Consent practices and audio-recording rules also depend on state law, so the legal layer needs counsel, not just engineering. Compliance is a design requirement from the start, not a feature added later.
Can a telesitter see or record everything in the room?
Well-designed platforms don’t. Many run live-only, storing no footage at all, and all should offer a one-tap privacy pause or masking mode so the observer blanks the feed during exams and private care. Devices carry visible indicators showing when the camera is active. A custom build can go further — automatic bed-zone masking or a stick-figure view that shows posture without a recognizable image.
How is a telesitter different from an AI fall detection camera?
A telesitter puts a human observer in the loop, watching live and intervening by voice; an AI fall detection camera tries to detect a fall automatically and alert without a person watching. They’re complementary: AI cues can direct a human observer’s attention, but at hospital scale a purely automated detector produces too many false alarms to trust alone, which is why virtual observation keeps a person making the call.
What to read next
Healthcare
Remote Patient Monitoring Platforms
The vitals-and-devices side of home care — the natural partner to in-room video observation.
Computer vision
AI Fall Detection Cameras
The automated-alert cousin of a telesitter — how detection works and where it stops.
Compliance
HIPAA-Compliant Video Platform
The privacy and security foundation any patient-facing video system has to sit on.
Security
Secure Video Communication Apps
Encryption, access control, and audit — the engineering behind a trustworthy feed.
The bottom line on virtual patient observation
A telesitter platform earns its place by turning one-to-one watching into one-to-many, and the independent evidence says it reliably cuts sitter cost and usually cuts falls. But the value isn’t in the camera — it’s in the escalation path that gets a nurse to the bedside in time, and the privacy design that keeps a patient’s room from becoming a liability. Build those two layers well and everything else is refinement.
Buy a platform when you want fewer falls this quarter; buy a service when staffing the hub is your real problem; build when integration, data residency, or product ownership makes observation strategic. If you’re not sure which side of that line you’re on, we’ll help you decide before you commit — you can book a 30-minute call or explore our video surveillance development services and telemedicine work to see where we’d start.
Let’s scope your telesitter platform
Whether you’re choosing a vendor or building observation into your own product, we’ll give you an honest read in 30 minutes — buy or build, with the integration, privacy, and cost tradeoffs to back it.









